
Bringing MOCHA Lessons to Your Service
Issues and Opportunities in Primary Health Care for Children in Europe
ISBN: 978-1-78973-354-9, eISBN: 978-1-78973-351-8
Publication date: 6 May 2019
Abstract
Identifying the qualities of primary care that have the potential to produce optimal health outcomes is only half the story. The Models of Child Health Appraised (MOCHA) project has not only explored how to transfer these to other national contexts, but also which successful components should be transferred. It is important to assess the population criteria of the identified sociodemographic, cultural and social characteristics and the population perspectives on a care system’s components. The project analysed public experiences and perceptions of the quality of primary care for children from a representative sample of the general public in five European Union member states. The public perception of children’s primary care services, in particular the perceived quality of care and expectations with regard to care for children, is important to understand before MOCHA lessons can be effectively adopted in a country. We found that the socio-cultural characteristics of a country inform the population perceptions and preferences with regard to the care system. In the five countries surveyed, there was agreement about aspects of quality of care – such as accessible opening hours, confidential consultations for children and timeliness of consultation for an illness, but there was a difference in opinion about giving priority to items such as making an appointment without a referral, or a child’s right to a confidential consultation. The cultural context of transferability and the means of addressing this such as defining the target audience and the different means of disseminating important messages to the wider community to address contextual factors can act as barriers or facilitators to the introduction of new components of primary care models.
Keywords
Citation
Boere-Boonekamp, M., Groothuis-Oudshoorn, K., Schloemer, T., Schröder-Bäck, P., van Til, J., Zdunek, K. and Kocken, P. (2019), "Bringing MOCHA Lessons to Your Service", Blair, M., Rigby, M. and Alexander, D. (Ed.) Issues and Opportunities in Primary Health Care for Children in Europe, Emerald Publishing Limited, Leeds, pp. 359-370. https://doi.org/10.1108/978-1-78973-351-820191006
Publisher
:Emerald Publishing Limited
Copyright © 2019 European Commission
License
This chapter is published under the Creative Commons Attribution (CC BY 4.0) licence. Anyone may reproduce, distribute, translate and create derivative works of this chapter (for both commercial and non-commercial purposes), subject to full attribution to the original publication and authors. The full terms of this licence may be seen at http://creativecommons.org/licences/by/4.0/legalcode
Introduction
The Models of Child Health Appraised (MOCHA) project has identified the qualities of primary care health systems that have the potential to produce optimal health outcomes for children in European Union (EU) countries. The question can then be asked what successful components of a care system should be transferred from one country to another. For instance, to reach accessible services with child friendly opening hours (see Chapter 11), or continuous professional–client relationships responsive for a child’s changing needs. MOCHA developed a long list of criteria for assessing this transferability. The criteria have been summarised in a population characteristics, intervention content, environment and transfer – transferability (PIET-T) process model (see Chapter 16) (Figure 18.1) (Schloemer & Schröder-Bäck, 2018). This chapter focuses on the population criteria for transferability, including sociodemographic, cultural and social characteristics, the population’s perceptions of health and health services and the population’s attitude towards the care system’s components.
The public perceptions and preferences included in the PIET-T model are vital. MOCHA conducted a client preference study among EU citizens of five countries to obtain insight into the public’s perceptions and attitudes of the care systems in a selection of EU countries (Van Til, Groothuis-Oudshoorn, & Boere-Boonekamp, 2018). The perceptions of primary health care services imply that the public builds preferences on the basis of the experiences with the system (see the P section of Figure 18.1). Public perceptions have been shown to be important for transferring new methods of primary care delivery.

Principles of Transferability with Special Attention to Influences from the Perspective of the Public
In order to bring MOCHA lessons to your service, it is essential to identify, discuss and – ultimately – apply evidence-based good practice and implement these in new contexts. This idea of good or best practice exchange in health care is a main principle of EU Public Health. With limited directive power, the European Commission has the potential to facilitate such good or best practice exchange and stimulate in such a way the improvement of health care across the EU. The identification of good and best practices – a lead task for DG SANTE but also for research projects within the Horizon 2020 scheme such as MOCHA – is thus of great importance. In addition to research, Commission activities exist to support the identification and exchange of good and best health practices research. However, to identify a good or best practice in one context (e.g. in one EU member state) does not mean that this practice will also be effective if implemented in another context (e.g. in another EU member state). To give a concrete example, compulsory measles immunisation might be effective and a best practice in some countries (as is the case in Czech Republic and Hungary) and might be introduced in other EU member states but it remains to be seen if it is effective in that country and may well be an unacceptable option for other EU countries.
The concept of transferability is crucial to any good and best practice exchange, yet, relatively little research exists that supports the understanding of transferability of health interventions in European public health and offers tools to facilitate this. The MOCHA project has aimed to identify validated criteria to inform transferability of good and best practices.
An explorative analysis of facilitators and barriers in setting effective policies, considering good and best practice exchange, and a systematic review resulted in the creation of two models of transferability (Schloemer & Schröder-Bäck, 2018). Firstly, the conceptual PIET-T describes, from the perspective of decision and policy-makers, the primary context (in which evidence of good and best practices were gained) and the target context, to which these practices shall be transferred and in which they could be implemented. Contexts in this regard could be different EU countries, but also smaller-scale contexts, such as cultural, administrative region, provinces or municipalities.
A second model created was the Process Model for the Assessment of Transferability. This model presents – in accordance with the conceptual model – the criteria of transferability grouped under four headings:
- (1)
population characteristics;
- (2)
intervention characteristics;
- (3)
environmental characteristics; and
- (4)
aspects of transfer.
These criteria help determine which information is relevant for the target context and allow a comparison with existing information on the primary context. By assessing these criteria, we can identify facilitators and barriers. However, transferability cannot be measured using existing information from this phase, but can only be anticipated. To make these criteria operational, a detailed overview of descriptive themes, criteria and subcriteria is essential. To this end, we have created a checklist tool (Schloemer & Schröder-Bäck, 2018). This model reflects themes related to population that play a role in the (non)implementation of good and best practices, because they can facilitate or inhibit transferability. The term population here mainly refers to the potential recipients of child primary health care and related persons in a country. We therefore underline the population themes with a focus on the public’s perceptions of children’s primary healthcare services, in particular perceived quality of care. Furthermore, acceptability is an important criterion, and so, we emphasise public preferences with regard to child primary health care. Our third focus is on cultural population characteristics as these may vary greatly depending on the specific context and might influence transferability of services. These aspects of the population are highlighted in italics in Figure 18.1.
Public Experiences and Priorities in Primary Care for Children
In order to create optimal primary care for children, the views of all stakeholders on which changes are necessary and are achievable in policies are of utmost importance. This includes the opinions of citizens. Data on citizens’ experiences and preferences are described in the Population part of the PIET-T process model of Schloemer and Schröder-Bäck (2018) (Figure 18.1) and can be used to estimate whether strengths in one country can be transferred to another country.
We elicited public experiences and perceptions of the quality of primary care for children using a cross-sectional study and a representative sample of the general public (Van Til et al., 2018) (see Chapter 3). We also asked about priorities of primary care in respect of children. These tasks are shown in Figure 18.1, in the section entitled Preferences. The following countries were chosen for this study:
the United Kingdom and the Netherlands (both GP-led system with GP gatekeeper to other healthcare services);
Germany and Spain (both primary care paediatrician-led, respectively, open access to secondary care and gatekeeper); and
Poland (mixed system and gatekeeper).
The questions in the Preferences For Child Health Care Assessed (POCHA)-questionnaire were related to nine potential quality attributes of a primary care system from child-, youth- and carer-centred perspectives: accessible, affordable, appropriate, confidential, continuous, coordinated, empowering, equable and transparent (Van Til et al., 2018).
In total, 2,403 respondents filled out the questionnaire: 469 from Germany, 469 from the Netherlands, 478 from Poland, 491 from Spain and 496 from the United Kingdom. Of all respondents, 36.3% had one or more children below 18 years of age, 23.3% had older children, and 40.4% did not have children.
Experiences
Based on their experiences or perceptions, respondents indicated to what extent they were satisfied with the quality of primary care for children in their country, on a scale of 1 (very dissatisfied) to 10 (perfectly satisfied). Mean satisfaction scores differed significantly between countries, ranging from 5.5 (Poland) to 7.2 (Spain).
Each respondent rated the quality of the primary care system on ten out of 40 quality aspects (five-point Likert agree-disagree scale). The average agreement over all 40 items was highest in the Netherlands (70%), followed by the United Kingdom (68%), Germany (64%), Spain (62%) and Poland (56%). The item that was judged highest was the setting of the services being clean and appealing (range 73–84%). The item judged lowest was whether the child has the possibility to limit his parents’ access to his medical records (range 12–36%). For some items, the respondents’ perceived quality was comparable across countries, for instance that primary care facilities have ample opening hours (range 52–59%). For other items, there were large differences between countries, for example for a child’s right to have a confidential consultation with a primary care provider. Agreement scores for these items were consistently lower in Poland and Spain.
Priorities
For priority setting, we used a best–worst scaling case 1 methodology, with eight different sets of combinations of ten statements on quality items. Two random sets of ten statements were presented to each respondent.
Universal priorities for primary care for children according to respondents in this study are as follows: timeliness related to severity, adequate skills and competencies of practitioners; efficacy. Items which were consistently prioritised as low in all countries were as follows: convenient appointment system, the child’s possibility to limit their parents’ access to the child’s medical records and to express his opinions about his health management independently from his parents.
Each country also showed its very specific priorities, probably related to the country’s history and culture. For instance, very important to respondents in Poland was that children and/or their parents can make an appointment with other healthcare providers without a referral. In the top ten priorities in the Netherlands, there was the child’s right to a confidential consultation with the primary care provider. Finally, that a child’s health is not influenced by the parents’ background characteristics was very important to respondents from Germany, but less important in other countries.
Experiences versus Priorities
There were national differences in the public’s experiences and priorities. To account for this, we combined priority scores with experience scores for each country separately. This allowed the identification of areas of potential improvement based on the importance given to them by the respondents from that country. In Spain, for example, the potential for improvement was highest with regard to opening hours of primary care services and availability of specialised care (Table 18.1).
Overview of the quality aspects with a high potential for improvement, presented for each of the five countries.
| Country | Attribute | Quality Aspect |
|---|---|---|
| Germany | Continuous | All healthcare providers involved in the care of a child know about each other’s involvement, trust each other and work well together |
| Accessible | Primary care services for children have ample opening hours, the after-hour care arrangements are good enough, and home-visits are planned if needed | |
| Coordinated | If the main primary care provider of a child is not able to meet the needs of that child, that care can be given by other health professionals within the primary care practice | |
| Coordinated | If a child needs specialised and long-term care, hospitals and primary care providers collaborate to offer care close to the child’s home | |
| Affordable | The effort needed to get coverage and/or repayment for any out-of-pocket cost of primary care for a child is reasonable and feasible | |
| Netherlands | Appropriate | Primary care providers are able to dedicate enough time to working with a child |
| Accessible | Children and/or their parents know about the range of services available in primary care and how they can access them | |
| Poland | Continuous | All healthcare providers involved in the care of a child know about each other’s involvement, trust each other and work well together |
| Appropriate | In primary care, the facilities and equipment are available to deliver the services that are needed for children | |
| Accessible | Children and/or their parents can make an appointment with other primary care providers without a referral from the main primary care provider | |
| Coordinated | Specialised care (e.g. physiotherapy, dental health care, psychological care, specialised chronic care nurses) is available to a child within the primary care provider’s practice | |
| Accessible | Primary care providers provide care within a reasonable amount of time, given the severity of the health issue | |
| Spain | Accessible | Primary care services for children have ample opening hours, the after-hour care arrangements are good enough, and home-visits are planned if needed |
| Coordinated | Specialised care (e.g. physiotherapy, dental health care, psychological care, specialised chronic care nurses) is available to a child within the primary care provider’s practice | |
| United Kingdom | Continuous | All health care providers involved in the care of a child know about each other’s involvement, trust each other and work well together |
| Accessible | Primary care services for children have ample opening hours, the after-hour care arrangements are good enough, and home-visits are planned if needed | |
| Appropriate | Primary care providers are able to dedicate enough time to working with a child |
A major strength of this approach was that by combining priority scores with an evaluation of perceived quality, the most important areas of potential improvement in each country can be identified.
Cultural Aspects
Closely related to the PIET-T model criteria, research carried out by MOCHA explored the phenomenon of the culture of ‘evidence-based practice’ (Zdunek, Schröder-Bäck, Rigby, & Blair, 2018) and that the wider health policy is not only directed to the population, but that the population also drives the content of health policy. The work concluded that an awareness, acknowledgement and addressing of the contextual factors are essential for successful transfer of knowledge to another country or region. The importance of socio-cultural factors has been described in Chapter 17; here, we address their effect on policy-making and the most likely methods of transition across borders.
The MOCHA project conducted a survey of the project Country Agents (see Chapter 1) and also surveyed stakeholders in primary care services for children across the EU and EEA countries. For further details of the methodology, see Zdunek et al. (2018). What became evident in this research was that the content of policy varies from country to country, and, together with the analysis of contextual factors, forms a baseline for developing a map of the current status of child health care in Europe. Public awareness of child issues can be measured by the level of activity of actors who play the main role in the theatre of child health care (see Chapter 3). Two trends of approaching the contextual environment are the scientific approach and the institutional approach (see Figure 18.2).

This evidence is not valuable for transfer of knowledge to different service environments without considering its context. As our respondents commented in the survey:
it is also not always possible to meet all criteria of the evidence-based medicine to one hundred percent. In some subjects, this is also difficult - for example, in paediatrics. (Austrian CA)
We found that contextual factors, particularly the media in each country, were powerful factors in forming barriers or facilitating policy change. The Greek Country Agent, for example, stated that: ‘results and suggestions by the report [into problems in the primary care health system and suggestions for change] were used mainly through news media (TV and printed press), in facilitated discussions between representatives of the political parties, health professionals and administrative staff of the health system’ (Zdunek et al., 2018). The media in Romania played a significant role in national debates about vaccination – at the beginning of a phenomenon of vaccine refusal by many parents, the media were said to have a lack of neutrality, giving a prime-time voice to a number of anti-vaccination voices alone on media outlets, without giving opportunity for a pro-vaccination voice to facilitate debate through the plurality of opinions. The most challenged vaccinations were against measles and polio. However, after a measles epidemic occurred, a shift in risk perceptions was observed in the Romanian media, which became an important actor advocating in favour of vaccination. Journalistic campaigns began to report illness and death and pressured the government to take concrete measures to limit the epidemics.
The media not only promotes awareness of existing evidence, but also about awareness of context. For example, the Bulgarian CA stressed that:
the obvious truth is that the outcome of treatment of many chronic diseases depends on the effect of the medical measures, but depends also on the social environment in which these measures are undertaken. If these social factors are not taken into account, there is a high risk that the medical measures are not implemented. (Bulgarian CA)
In the MOCHA Stakeholder survey, we asked about the most influential stakeholders, who can play a strategic role in circulating recommendations about optimal models of child health care in Europe. The respondents concluded that the most respected and influential were medical and professional associations, as well as health professionals and patient organisations. These stakeholders not only are important in the circulation of the information, but also play a role in implementing the newly proposed solutions.
The stakeholders also concluded that transferability of knowledge was also achieved by a range of recommendations. A combination of new formal policies, guidelines and recommendations together with personal contact was seen as important. Seminars, conferences and workshops are significant facilitators of exchange of information, not only between countries but also between competent authorities. The experts highlighted the strategic role of media, including social media in the circulation of information about innovative solutions in terms of child primary health care. This facilitates the process of active implementation of proposed solutions.
What is important is to identify the most appropriate recipients for the new policy or idea in developing a new model. These take into account the agents of the child in the proximal and distal (wider) environment (see Chapter 4). What was found to be important was to match the format of recommendations to the audience profile, as one respondent commented, the format of advice ‘should be suited to the target audience’s profile, either individual or priority groups, that is peer-reviewed journal and/or seminar for stakeholders and professionals’, and another concluded that ‘implementation work must adapt to the relevant audience. Mostly reports, scientific publications, seminars and news items are either useless or make a temporary change. The format must appear useful for the person receiving it, and it must be followed up regularly to ensure actual implementation’ (see Zdunek et al., 2018).
The MOCHA data suggest there are several types of the most effective format for communicating scientific results. The scientific approach is relevant, popular and expected, accompanied by administrative and formal reports, strategies and recommendations. However, for successful transferability, as described in the PIET-T model above, data must be presented in an appropriate manner to the general population and those who are aware of the emerging possibilities of improvement in the quality of health care and health services. Thus, the media of television, radio, social media and other electronic media are also vital. Additionally, there is a need of public involvement in the discussion of newly proposed solutions. This is correlated with health education activities at the primary care level (see Chapter 11), health personnel (see Chapter 13), meetings with parents, young people and other citizens (see Chapter 3), decision-makers and public discussions. These different means of dissemination of knowledge and awareness of contextual and cultural factors is illustrated in Figure 18.3.
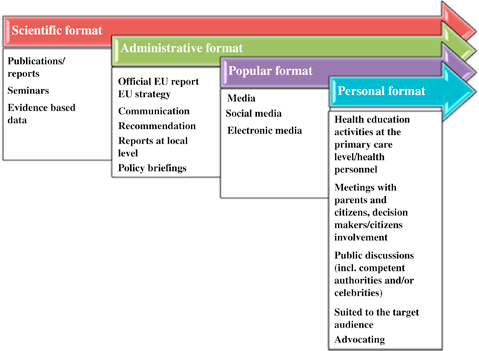
This proposed classification helps to adapt the format of the recommendations to the appropriate audience population, as shown in Figure 18.1. In the case of the audience in the proximal environment, a popular and personal format may be the most relevant. The audience in the distal environment would probably benefit more from the scientific and administrative format of data.
Summary
The implementation of a good or best practice from one country to another depends on many factors, which are described in the PIET-T process model of Schloemer and Schröder-Bäck (2018). The MOCHA project designed this model to compare the countries’ receptivity for inclusion of optimal features of care systems that have demonstrated improvement of quality of primary health care for children. This chapter focused on the Population section of the model. Public’s perceptions of children’s primary healthcare services, particularly perceived quality of care, and preferences with regard to child care services, will influence the transferability of services, depending also on socio-cultural characteristics of the population.
A study into the preferences of a representative sample from the general public of five EU countries showed that there was a difference between countries and also within countries in agreement about experiences with quality aspects of the primary care system, such as accessible opening hours or confidential consultations for children. Items such as timeliness related to severity of an illness were prioritised highly by all countries while countries differed in terms of giving priority to items such as making an appointment without a referral or a child’s right to a confidential consultation. The socio-cultural characteristics of a country seem important for these population’s perceptions and preferences with regard to the care system. The citizen’s experiences and priorities, which are described in the Population part of the PIET-T process model, are relevant for estimating whether care systems’ strengths in one country can be transferred to another. This can be done by comparing the PIET-T data of combinations of countries, as important differences might influence transferability. In this way, facilitators and barriers for transferability can be determined by analysing context-relevant criteria shown in Figure 18.1. Finally, we looked at the importance of the cultural context of transferability, and means of addressing this, defining a target audience and the different means of disseminating important messages to the wider community, and so addressing the contextual factors that can act as barriers or facilitators to knowledge transfer.
References
Schloemer & Schröder-Bäck (2018) Schloemer, T. , & Schröder-Bäck, P. (2018). Criteria for evaluating transferability of health interventions: A systematic review and thematic synthesis. Implementation Science, 13(1), 88. doi:10.1186/s13012-018-0751-8
Van Til, Groothuis-Oudshoorn, & Boere-Boonekamp (2018) Van Til, J. , Groothuis-Oudshoorn, K. , & Boere-Boonekamp, M. M. (2018). Public priorities for primary child health care for children. A report on public preferences for patient-centred and prevention oriented primary child health care models for children. Retrieved from http://www.childhealthservicemodels.eu/publications/technical-reports/
Zdunek, Schröder-Bäck, Rigby, & Blair (2018) Zdunek, K. , Schröder-Bäck, P. , Rigby, M. , & Blair, M. (2018). The culture of evidence-based practice in child health policy – A report. Retrieved from http://www.childhealthservicemodels.eu/publications/technical-reports/
- Prelims
- Chapter 1 The MOCHA Project: Origins, Approach and Methods
- Chapter 2 Models of Primary Care and Appraisal Frameworks
- Chapter 3 Listening to Young People
- Chapter 4 Child Centricity and Children’s Rights
- Chapter 5 Equity
- Chapter 6 The Limited Inclusion of Children in Health and Health-related Policy
- Chapter 7 The Invisibility of Children in Data Systems
- Chapter 8 The Conundrum of Measuring Children’s Primary Health Care
- Chapter 9 Measurement Conundrums: Explaining Child Health Population Outcomes in MOCHA Countries
- Chapter 10 Services and Boundary Negotiations for Children with Complex Care Needs in Europe
- Chapter 11 School Health Services
- Chapter 12 Primary Care for Adolescents
- Chapter 13 Workforce and Professional Education
- Chapter 14 e-Health as the Enabler of Primary Care for Children
- Chapter 15 Affiliate Contributors to Primary Care for Children
- Chapter 16 The Transferability of Primary Child Healthcare Systems
- Chapter 17 National and Public Cultures as Determinants of Health Policy and Production
- Chapter 18 Bringing MOCHA Lessons to Your Service
- Chapter 19 Evidence to Achieve an Optimal Model for Children’s Health in Europe
- Appendix 1: List of MOCHA Scientists
- Appendix 2: List of MOCHA Country Agents
- Index