
Child Centricity and Children’s Rights
Issues and Opportunities in Primary Health Care for Children in Europe
ISBN: 978-1-78973-354-9, eISBN: 978-1-78973-351-8
Publication date: 6 May 2019
Abstract
The child is at the centre of all Models of Child Health Appraised research and indeed all primary care delivery for children. Appraising models of primary care for children is incomplete without ensuring that experiences of primary care, design, treatment, management and outcomes are optimal for the child. However, the principle of child centricity is not implicit in many healthcare systems and in many aspects of life, yet it is extremely important for optimal child health service design and child health. By exploring the changing concept of ‘childhood’, we understand better the emergence of the current attitude towards children and their role in today’s Europe and the evolution of child rights. Understanding child centricity, and the role of agents acting on behalf of the child, allows us to identify features of children’s primary care systems that uphold the rights of a child to optimum health. This is placed against the legal commitments made by the countries of the European Union and European Economic Area to ensure that children’s rights are respected.
Keywords
Citation
Zdunek, K., Rigby, M., Deshpande, S. and Alexander, D. (2019), "Child Centricity and Children’s Rights", Blair, M., Rigby, M. and Alexander, D. (Ed.) Issues and Opportunities in Primary Health Care for Children in Europe, Emerald Publishing Limited, Leeds, pp. 77-98. https://doi.org/10.1108/978-1-78973-351-820191009
Publisher
:Emerald Publishing Limited
Copyright © 2019 European Commission
License
This chapter is published under the Creative Commons Attribution (CC BY 4.0) licence. Anyone may reproduce, distribute, translate and create derivative works of this chapter (for both commercial and non-commercial purposes), subject to full attribution to the original publication and authors. The full terms of this licence may be seen at http://creativecommons.org/licences/by/4.0/legalcode
Introduction – A Challenge for Policy-makers
The child is at the centre of all Models of Child Health Appraised (MOCHA) research. Appraising models of primary care for children is impossible without ensuring that experiences of primary care, treatment, management and outcomes are optimal for the child. When designing child health systems, it is easy to focus on the population level and on the needs of the majority adult population, but this risks devaluing the status of the child. Children make up a quarter of the population and are frequent users of primary care – not least for preventive services (Blair, Rigby, & Alexander, 2017). The principle of child centricity is not implicit in many healthcare systems and in many aspects of life, yet it is extremely important for optimal child access and child health. This chapter explains the objective and philosophy of child health service provision in MOCHA. Understanding true child centricity is logically an essential prerequisite to the design and provision of optimal child health services. Even certain aspects of the MOCHA mission, in emphasising that children are the future of society, risk a societal utilitarian approach – healthy children are seen as a ‘good thing’ as they will metamorphose into a healthy adult population, boosting economic and societal strength and gain. The challenge is to make the child the focus, from a local to international level. A child is considered important as a member of society, as evidenced by the European Values Survey (2015) (see Chapter 17), but this is not necessarily represented in societal structures.
The Child in a Socio-cultural Context
How can a child and childhood be considered as the prime value in a child-centric paradigm embedded in the European socio-cultural context? History shows that the attitudes towards the child have changed throughout the ages. These changes are the consequence of socio-cultural shifts in the perception of the child as an intrinsic rather than an extrinsic value. Socio-cultural contexts have altered attitudes towards children and created their value in society, including towards their health. Culture, which is understood as the results of human actions in terms of material and ideal concepts, values and accepted ways of doing things, is objectified and accepted by collectives and transferred to other collectives and next generations (Szczepański, 1963) (see also Chapters 16 and 17). Culture plays a regulatory role towards behavioural aspects in changing multicultural Europe.
The Changing Concept of a Child and the History of Rights Approaches
The concept of the child and childhood has been changing in terms of time, place and space (Garbula & Kowalik-Olubińska, 2012). In Ancient Greece, the child was obliged to yield to his or her father’s will. Spartan children were considered to be the property of the state, which was supposed to take care of their physical and military development (Rosa & Matysiuk, 2013), in a system known as agoge (Kulesza, 2003). Aristoteles identified the need to care for children’s intellectual and physical development and health as it was common that disabled children, or those who were born in an extramarital relationship or orphaned, were often condemned to a life of ostracism and poverty (Rosa & Matysiuk, 2013). In Ancient Rome, the father had the right to decide about the life and death of a child by law (Rosa & Matysiuk, 2013). A change in attitudes towards children came in the Middle Ages. Ariés (1962) describes the Middle Ages as a time when a child was seen solely as a small adult; but this view contrasts with research conducted by other medievalists (Brzezinski, 2012). The perception of a child at that period in Europe was strongly influenced by the image of the child presented in the Christian Bible; expressed, for example, by the privileged access of children to the kingdom of God (Brzeziński, 2012). The child, thus, became an object of value and the family became responsible for his or her social and moral development (Rosa & Matysiuk, 2013). Ibrahim ibn Yaqub, in the tenth century, wrote that in Slavic countries, a soldier was even paid his wages on the day of his child’s birth, whether it was male or female. The Renaissance (1350–1700) saw greater appreciation of the personality of a child. Attention was given to poor children, who benefited from public education. Additionally, the idea of Erasmian humanism ‘conceived of education as a method for cultivating human potential and dignity to the fullest possible extent’ (Parrish, 2013). The enlightenment of the eighteenth century (1685–1815) attached great significance to the institutionalisation of care directed at excluded and marginalised children. John Locke (1632–1704) played a significant role and claimed that ‘the child has needs and interests which should be recognised for what they are and that the child should be reasoned with, not simply beaten or coerced into conformity with the ruled of required behaviour’ (Archard, 2004). The French Revolution at the end of the eighteenth century marked a point when children were first given rights and parents were obliged to protect the child. Social development, as well as the development of humanism and respect of the individual, was mirrored in the ideas of the French Revolution and the attitudes of the Christian Church claiming that the child has its own rights and lack of respect to them was considered a sin (Jarosz, 2010). However, the industrial era of the nineteenth century in Europe saw new challenges for children. Children suffered high mortality and poor living and working conditions, and they were used as sources of cheap labour (Balcerek, 1986), There was an increased level of juvenile delinquency as the consequence of this lack of care. Initiatives which aimed to care of the homeless and abandoned children, debates on juvenile courts and moral education of children prompted a fundamental change in terms of philanthropic activities in the nineteenth and twentieth centuries in Europe (Balcerek, 1986), which were effectively the first steps in the development of children’s rights.
The beginning of twentieth century brought the emergence of protection and educational initiatives directed at children. Organisations such as Save the Children in England, Rädda Barnen in Sweden and the International Save the Children Union (UISE) were established to protect and educate children. In 1924, the League of Nations inspired by UISE adapted the Geneva Declaration of the Rights of the Child to protect vulnerable children and victims of the war. We could consider it as a first step in empowering the child as an actor in society; in effect, from this point onwards, it could be argued that this is when the child began to be considered as a value in itself, rather than solely as parents’ or state property. This was an important milestone in the recognition of the children rights (see Box 4.1).
The Geneva Declaration of the Rights of the Child.
“By the present Declaration of the Rights of the Child, commonly known as “Declaration of Geneva,” men and women of all nations, recognizing that mankind owes to the Child the best that it has to give, declare and accept it as their duty that, beyond and above all considerations of race, nationality or creed:
The child must be given the means requisite for its normal development, both materially and spiritually;
The child that is hungry must be fed; the child that is sick must be nursed; the child that is backward must be helped; the delinquent child must be reclaimed; and the orphan and the waif must be sheltered and succoured;
The child must be the first to receive relief in times of distress;
The child must be put in a position to earn a livelihood, and must be protected against every form of exploitation;
The child must be brought up in the consciousness that its talents must be devoted to the service of fellow men.”
Further recognition of a child’s rights in the second half of the twentieth century is evidenced by increasing legal recognition of the place of a child in society. Table 4.1 shows the key important events, culminating in the 1989 UN Convention on the Rights of the Child (UNICEF, 1989) which is signed by all MOCHA countries and should inform all aspects of children’s health care to this present day.
Timeline of increasing awareness and respect for the rights of a child in Europe.
| 1946 | The United Nations International Children’s Emergency Fund (UNICEF) and the United Nations Educational, Scientific and Cultural Organization (UNESCO) are created |
| 1948 |
The Universal Declaration of Human Rights is created. Included in article 25 is a statement that makes children’s rights equal whether a child is born to married or unmarried parents
|
| 1948 |
Declaration of the Rights of the Child (United Nations, 2015) supplemented the Geneva Declaration of the Rights of the Child. Two points were added as the consequence of the experiences of the Second World War:
|
| 1950 | European Convention on Human Rights, which in Art 5, states that ‘Spouses shall enjoy equality of rights and responsibilities of a private law character between them, and in their relations with their children’ (Council of Europe, 1950) |
| 1959 |
The Declaration of the Rights of the Child is produced by the United Nations. This document stresses the importance of child health and in particular the role of the Agents of the Child in the process of care
|
| 1961 | European Social Charter (Council of Europe). This charter gave recognition to the care of the mother and child: the Right to social protection for mother and child and the Right of children and young persons to protection (Council of Europe, 1961) |
| 1966 |
International Covenant on Civil and Political Rights. This covenant contained:
|
| 1976 |
International Covenant on Economic, Social and Cultural Rights
|
| 1989 | UN Convention on the Rights of the Child |
Art. 3.
|
The Child-centric Paradigm and the Child as an Actor in Health Care
The current recognition of child rights is evidence of the emergence of the concept of the child as an active actor in society. Bronfenbrenner (1979) theorised that development and socialisation of child are affected by linkages on micro-, meso-, exo- and macro-levels. Bronfenbrenner’s theory requires the acceptance of the following assumptions:
Person is an active player, exerting influence on his/her environment.
Environment is compelling the person to adapt to its conditions and restrictions.
Environment is understood to consist different size entities that are place one inside another, of their reciprocal relationship and of micro-, meso-, exo- and macro-systems (Bronfenbrenner, 1979; Härkönen, 2007).
We propose to adapt this frame into a child-centric paradigm in health care by:
considering the child as an active player empowered in the process of healthcare provision but also in defining health policy via the agents of the child;
the child is embedded in particular environment which requires to adapt and respect the common principles and values; and
the environment will be understood as the wider context of socio-cultural, structural, external and internal background which will interact between child and its proximal and distant environment on different levels.
This is explained in more detail in Figure 4.1.

In order to achieve truly child-centric healthcare systems, it is important not only to consider the individual child, but also to look wider to population measures that benefit the individual. This is where child-centric health policy-making is vital. Policy-making and implementation do not happen in isolation, but are always embedded in a broader societal context which includes both systemic and socio-cultural elements (see Chapter 17). Initiatives in health policy are not only directed to the population but also driven by the population, including the needs of children (see Chapter 17). Walt and Gilson (1994) applied a triangle framework to describe the paradigm of policy analysis, in which the attention is not only focused on its content, but also on the processes affecting the development and implementation of the change, the context within which policy is created and the actors involved (Walt & Gilson, 1994). Context in our understanding refers to systemic factors (Buse, Mays, & Walt, 2005). It can be considered through the perspective of four factors: situational, structural, (socio)cultural and international (adapted from Buse et al., 2005; Leichter, 1979) (see Figure 4.1). We consider it as extremely useful to child-centric policy-making thus it formed an important part of the MOCHA research on appraisal of primary care systems from a child-centric perspective. Our assumption was to consider the child as an actor in the theatre of child health policy in European countries.
MOCHA research has identified that children are the main object (both direct and indirect) of disputes related to child health care across most European countries in the last decade. In this context, a child as an object of a child-centric health policy is either a well child (embedded in the family context, broadly understood social environment context or preventive care context) or a sick child (with a long-term illness and/or complex healthcare needs). Heterogeneity is expressed also by the differentiation of the child health issues in various age groups (from pre-natal period via infancy to adolescence).
The Concept of an ‘Agent’ for the Child
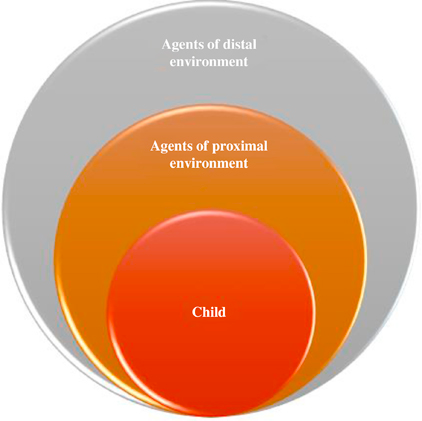
In most discussions on child health policy, the child is not an active participant in discussions even though a child is the subject and often the cause of a societal movement or change in policy; in other words, the child is a causative actor. As such, the child is surrounded by an extensive network of representatives. These actors are able to act and represent the interest of the child and are thus defined as executive actors. These individuals, who may be parents, teachers, nurses, physicians or other adults, can be considered as agents of the child in the proximal or distal environment of the child. The proximal environment of the child is defined as the micro-level, or the direct milieu of the child’s environment (such as a parent or other family member); distal environments are defined as the indirect surroundings, on the mezzo- and macro-level. The difference between the distal and proximal environment of the child is expressed by the type of relationship. In the proximal perspective, the agents are capable of constructing a direct relationship whereas the agents of the distal environment are generally acting on the basis of indirect contact. This is illustrated by Figure 4.2.
Agents of the Proximal Environment
This group includes parents, close family members and others who have close contact with the child, such as teachers, nurses and physicians. Parents are vocal in their role as a child’s representative and, in many situations, are supported by involved caregivers within social care and healthcare services. Parents, more often than other agents, are considered as both causative and executive actors. For instance, policy in Austria concentrates on helping pregnant women and new mothers to cope with the challenges of early childhood (ages 0–6) and puts in place guidance through the health and social care system in that country. Parents are also central in the role of advocating for the rights of their child, in countries where there is compulsory vaccination, parents have raised objections to the potential marginalisation of children who have not been vaccinated; arguments both for and against the policy have featured parent voices very strongly (see Zdunek, Schröder-Bäck, Alexander, Rigby, & Blair, in press) (see Chapters 16 and 17). Agents of the child in the proximal environment may also include other people who closely surround the child, such as family members, acquaintances, friends, neighbours, adults in the school environment as well as general practitioners or other representatives of health care who are the ‘listeners’ and ‘observers’ institutionally empowered to act in the name of the child. It was teachers who raised awareness of children in Greece who, as a result of extreme austerity measures in that country, were fainting at school because of hunger, causing a national scandal, and in Spain, schools became part of anti-poverty measures by keeping their canteens open during the summer holidays to ensure children would be able to eat a meal (see Zdunek et al., in press ).
Agents of the Wider Environment
The distal (wider) environment is where agents of the child become more closely entwined in national policy and population-level perspectives, while being child-centric in outlook. Examples of such agents include healthcare professionals’ representative of the healthcare system as a whole, non-governmental organisations (NGOs) and research and media outlets. An institutional voice can take the form of, for example, health inspectorates, professional groups, children’s health centres, national agencies and public health institutions. For example, paediatricians’ associations were actively involved in the public discussion on changes to vaccination eligibility in Spain, and nursing associations in Norway were active in the introduction of weighing and measuring children at school as an obesity prevention policy (see Zdunek, Schröder-Bäck, Blair, & Rigby, 2017).
NGOs can be the platform for the exchange of views for health professionals, parents and carers and other interested persons who wish to ensure the protection of child health and well-being is protected. For example, in the UK, charities and organisations have strongly criticised the absence of a coordinated response to meet the needs of unaccompanied asylum seeking children in the country (Zdunek, Schröder-Bäck, Blair, & Rigby, 2017). Representatives of government such as the Ministry of Health (MoH) or other national institutions can also act as distal agents of the child. They can play the role of initiator of a policy, or be a mediator or guardian in a debate even though they are, by the definition, the ‘voice of the state’.
An important example of a distal agent of the child is that of individual authorities, such as an ombudsman for children’s rights. The individuals and their departments directly advocate for children’s rights, whether it is in terms of child abuse, disabilities, unaccompanied asylum-seekers or disabled children’s rights (for further details, see Zdunek, Schröder-Bäck, Blair, & Rigby, 2017).
A crucial role is also played by research centres and the mass media as sources of information and means of dissemination about certain phenomena. The media, in particular, can play a dual role, in terms of identifying and disclosing information about an issue; they are powerful instruments in public discussion. It was investigative journalism in Romania that exposed a potential scandal in children’s residential home, where 12 out of 28 children aged between six and 16 had been administered narcoleptic medication for behavioural disorders, despite the fact that the facility was not a special needs centre, but housed children at risk, or abandoned children (mostly because of family poverty) (Blair et al., 2017). Public outcry led to an investigation that found, in this case, that the medication had been medically prescribed.
Children’s Rights to Health
Meanwhile, society can discharge a focus and responsibility for children by acknowledging the need to frame what the child can expect from society as declaration of rights. These are intended both to define the child’s interests and to discharge society’s duty of care as distal agent. The study of how to collate aspects of children’s rights into meaningful service provision-related statements has been led by Michael Rigby and Shalmali Deshpande, linking also to other work such as the World Health Organization’s initiatives.
Core Concepts of Children’s Right to Health
Recognition of Children’s Rights is an important enablement and policy tool which seeks to give authenticity and impact to child centricity. Given that the child, as a legal minor, cannot advocate for themselves, and not every parent or service provider can be guaranteed to act optimally, giving legal underpinning to the rights of children gives a clear framework, and a yardstick against which failures can be judged, and redress applied where appropriate. It is an approach strongly supported at the highest level by the European Commission, through the Fundamental Rights Agency (2018) (which covers all ages) and by the Rights of the Child unit within DG Justice and Fundamental Rights (2018).
However, within this commitment to children’s rights, health is a complex paradox. Firstly, there is the definitional problem. An oft cited key principle is the Right of the Child to Health, as enshrined in the United Nations Declaration on the Rights of the Child (United Nations OHCHR, 1959). However, the wording is aspirational and laudable, but lacks any meaningful definition, as being:
States Parties recognize the right of the child to the enjoyment of the highest attainable standard of health and to facilities for the treatment of illness and rehabilitation of health.
There are no measurable benchmarks or definitions within that aim. Secondly, the provision of health services is a national competence under EU law, and so each country has its own approach to healthcare provision – deepening the measurement challenge as shown throughout the MOCHA project.
As for Health itself, that too is challenging to measure. The Constitution of the World Health Organization (World Health Organization, 1946) provides the authoritative definition, as being:
Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.
Clearly, to measure that for children through the life course is a daunting challenge. Though recognising that there are some contributors such as the Health Behaviour of School-aged Children (2018), these are not widespread or detailed enough to provide a systematic monitoring of fulfilment of the Right to Health.
The further challenge to the MOCHA project is that the project focus is on primary care for children. As shown throughout the report, primary care is delivered in different ways in different countries and by different people. There are also many reasons for providing health care – for preventive services, for diagnosis and treatment of a health problem at an early stage and for responding to health emergencies. The Right to Health should apply to all these circumstances, within any country’s healthcare system, and regardless of individual circumstance. All countries will claim to provide such services universally to their citizens and usually to their residents, but in practice, there may be variation in provision or in accessibility according to locality or socio-demographic, cultural or ethnic factors, as discussed in Chapter 5. One specific aspect to this complexity concerns primary care provision for migrant and refugee children, and a focussed investigation within MOCHA addressed and researched this in detail and highlighted problematic areas (Hjern & Østergaard, 2017). However, important though rights and equity are for migrant and refugee children, this does not assist with the problem of assessing achievement of the Right to Health for resident children.
Appraisal of the Right to Health
The conclusion of the MOCHA team is that a more meaningful expression of the Right of the Child to Health, not least within primary care, is needed, giving practical operational instantiation to the high-level right. The World Health Organization Regional Office for Europe has previously started an initiative to enable countries to assess whether children are receiving the health care thought appropriate, based on the broad concepts in the United Nations Convention on the Rights of the Child turned into provision-based aspects. A toolkit has been produced with tools aimed at 6 − 11-year-old children, 12–18-year-old children and separately for management, health professionals and parents and carers (World Health Organization, 2015). These tools assess whether in the respondent’s view good practice is being followed in order to facilitate the child’s right to health through good primary care, but the questions themselves are only indirectly derived from Rights statements. This initiative builds on a successful initiative looking at Children’s Rights in Hospitals and a related toolkit, but so far, the primary care toolkit has only been piloted in two countries in Europe (Guerreiro, Kuttumuratova, Babamuradova, Atajanova, & Weber, 2015). As presented, it is a local use initiative, and there is no infrastructure for comparison between states.
The MOCHA project has looked at assembling a more comprehensive grouping of all children’s documented rights relating to health and in accord with enabling and achieving the core Right to Health. There are several relevant treaties or consensus statements which have one or more items relevant to affecting the Child’s Right to Health. All the sources selected are legally binding treaties or potentially robust European policy statements which can be analysed as supporting aspects of children’s primary healthcare delivery. There is recognised to be a hierarchy of conventions, treaties and agreements. Those which are legally binding international conventions are the strongest in that countries agree at governmental level to ratify them as a nation, after which they are bound to uphold them. Second, within the European Union, Commission Directives are the strongest form of instrument and are arrived at after due process of discussion and agreement and are legally binding on Member States. A third and lower level of impact can be achieved when Ministers of Health meet on a special topic and mutually agree principles. These are not legally binding, but usually are based on sound evidence plus mutual solidarity and can provide useful benchmarks and levers for ensuring that countries keep to agreed principles. These latter types of agreement can be reached globally, or within global regions such as Europe.
Based on this hierarchy, the MOCHA project has identified four instruments which when linked together can give more detailed expression of the Rights of the Child to Health within primary care. These are as follows:
International conventions – there are two which are relevant:
- (1)
Universal Declaration of Human Rights (United Nations, 1949); and
- (2)
United Nations Convention on the Rights of the Child (United Nations, 1924)
- (1)
EU directives – none were identified pertaining to children’s primary health care;
Ministerial convention declarations – at global level Declaration of Alma-Ata, International Conference on Primary Health Care, 1978 (World Health Organization, 1978); and
Ministerial convention declarations – at European level Tallinn Charter: Heath Systems for Health and Wealth 2008 (World Health Organization Regional Office for Europe, 2008).
Based in decomposition of the child and primary care relevant content of these four agreements, and reassembly in a systematic and integrated manner, the project has synthesised 12 suggested Rights of Children to Primary Health Care, with supporting enabling statements. These are shown in Table 4.2 and are based in statements in the four source documents.
Rights of children to primary health care.
| Child Primary Care Rights Statement | Enabling Service Policy Statements (and Underpinning Source) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The project has also commenced a process of assembling underpinning evidence from scientific literature to support the approaches, but within the terms of reference and resources of the MOCHA project, it has not been possible to fully complete this work. A hypertext linked presentation has also been developed, enabling automated linkage from any listed Right to the underpinning authorising text and where compiled the related literature.
From this assemblage of the Rights of the Child to Primary Care, it will be possible to assemble means for monitoring policy and provision to achieve these rights. This should enhance the approach already commenced by the WHO European Regional Office.
More work remains to be done on defining and monitoring a Child’s Right to Primary Health Care, but this fundamental concept underpins the concept of child centricity and the Right to Health. There is need and opportunity to develop fully and obtain high-level agreement to these rights statements translated into practical service guidelines and to further developing monitoring tools, including child-friendly ones.
Summary
This section of study has traced the change in the perception of the child within society, from being a chattel of the father to being a person who should be nurtured, then from being an economic agent to being a developing person whose value to society will be achieved as a peak of optimal adulthood. Along this route, society has changed its views of the role of children and the duty of care from one of paternal protectionism to one of defining and actively supporting the child’s rights. And during that journey, the role of the health sector has moved from one of paternalistic protection, to one of protecting rights to protection and self-determination as an emergent citizen. Child centricity is simultaneously a recognition of the individual child’s importance in terms of rights and as a user of services and also as an agent of societal change. Using the example of children as actors in the creation of child health policy, we have looked at how and to what extent child centricity has been developed in Europe. The extent to which a system has the capacity to be child-centric is an important factor in the appraisal of primary care systems.
References
Archard (2004) Archard, D. (2004). Children. Rights and childhood. London: Routledge.
Ariès (1962) Ariès, P. (1962). Centuries of childhood: A social history of family life. London: Jonathan Cape.
Balcerek (1986) Balcerek, M. (1986). Prawa dziecka. Prawa dziecka Wydawnictwo Naukowe. Warszawa: PWN.
Blair, Rigby, & Alexander (2017) Blair, M. , Rigby, M. , & Alexander, D. (2017). Final report on current models of primary care for children. Retrieved from www.childhealthservicemodels.eu/wp-content/uploads/2017/07/MOCHA-WP1-Deliverable-WP1-D6-Feb-2017-1.pdf
Bronfenbrenner (1979) Bronfenbrenner, U. (1979). The ecology of human development, experiments by nature and design. Cambridge, MA: Harvard University Press. Retrieved from https://khoerulanwarbk.files.wordpress.com/2015/08/urie_bronfenbrenner_the_ecology_of_human_developbokos-z1.pdf
Brzeziński (2012) Brzeziński, W. (2012). Obraz dziecka w perspektywie historyczno-porównawczej. Przeszłość we współczesności, współczesność w przeszłości. Przegląd Pedagogiczny, 1(21), 141–153.
Buse, Mays, & Walt (2005) Buse, K. , Mays, N. , & Walt, G. (2005). Making health policy. Understanding public health. London: Open University Press.
Child Rights International Network (2018) Child Rights International Network . (2018). Declaration of the rights of the child 1948. Retrieved from https://www.crin.org/en/library/un-regional-documentation/declaration-rights-child-1948
Council of Europe (1950) Council of Europe . (1950). Convention for the protection of human rights and fundamental freedoms Rome, 4.XI.1950. In European convention on human rights. Strasbourg: Council of Europe. Retrieved from https://rm.coe.int/1680063765
Council of Europe (1961) Council of Europe . (1961). European social charter. Retrieved from https://rm.coe.int/168006b642
European Union Agency for Fundamental Rights (2018) European Union Agency for Fundamental Rights . (2018). About FRA. Retrieved from http://fra.europa.eu/en
European Values Survey (2015) European Values Survey . (2015). About EVS. Retrieved from https://europeanvaluesstudy.eu/
Garbula & Kowalik-Olubińska (2012) Garbula, J. , & Kowalik-Olubińska, J. (2012). Konstruowanie obrazu dzieciństwa w perspektywie psychologicznej i socjokulturowej. Przegląd Pedagogiczny, 1(21), 25–34. Retrieved from http://repozytorium.ukw.edu.pl/handle/item/626
Guerreiro, Kuttumuratova, Babamuradova, Atajanova, & Weber (2015) Guerreiro, A. I. F. , Kuttumuratova, A. , Babamuradova, M. , Atajanova, Z. , & Weber, M. W. (2015). Assessment and improvement of children’s rights in health care: Piloting training and tools in Uzbekistan; Panorama, 1, 3, 2015. Copenhagen: WHO.
Härkönen (2007) Härkönen, U. (2007). The Bronfenbrenner ecological systems theory of human development. In Slahova, A. et.al. (Ed.), Scientific articles of V international conference PERSON.COLOR.NATURE.MUSIC. Saule. Latvia: Daugavpils University. Retrieved from https://studylib.net/doc/8356343/the-bronfenbrenner-ecological-systems-theory-of-human
Health Behaviour of School-aged Children (2018) Health Behaviour of School-aged Children . (2018). HBSC. Retrieved from www.hbsc.org
Hjern & Østergaard (2017) Hjern, A. , & Østergaard, L. S. (2017). Migrant children in Europe: Entitlements to health care. Retrieved from http://www.childhealthservicemodels.eu/wp-content/uploads/2015/09/20160831_Deliverable-D3-D7.1_Migrant-children-in-Europe.pdf
Jarosz (2010) Jarosz, E. (2010). Krzywdzenie dzieci-piętno społeczne? (w) “CHOWANNA” 53 (66), T. 1 (34): DZIECIŃSTWO – WITRAŻ BOLESNY.
Kulesza (2003) Kulesza, R. (2003). Starożytna Sparta. Poznańskie Towarzystwo Przyjaciół Nauk, Mała Biblioteka PTPN t. 12, Pozdnań.
Leichter (1979) Leichter, H. (1979). A comparative approach to policy analysis: Health care policy in four nations. Cambridge: Cambridge University Press.
Parrish (2013) Parrish, J. M. (2013). Education, Erasmian humanism and more’s Utopia. In C. Brooke & E. Frazer (Eds.), Ideas of education: Philosophy and politics from Plato to Dewey. London: Routledge.
Matysiuk (2013) Rosa, R. , & Matysiuk, R. (2013). Ewolucja praw dziecka (aspekty filozoficzne, pedagogiczne i prawne). In E. Jagiełło & E. Jówko (Eds.), Dziecko w kulturze współczesnego świata (pp. 10–33). Siedlce ISBN 978-83-936635-2-1. Retrieved from https://docplayer.pl/4327137-Dziecko-w-kulturze-wspolczesnego-swiata-redakcja-naukowa-ewa-jagiello-ewa-jowko.html
Szczepański (1963) Szczepański, J. (1963). Elementarne pojęcia socjologii. Warszawa: PWN.
UNICEF (2003) UNICEF . (2003). Declaration of the rights of the child 1959. Retrieved from https://www.unicef.org/malaysia/1959-Declaration-of-the-Rights-of-the-Child.pdf
United Nations (1924) United Nations . (1924). Geneva declaration of the rights of the child. Retrieved from http://www.un-documents.net/gdrc1924
United Nations (1949) United Nations . (1949). Universal declaration of human rights. New York, NY: United Nations. Retrieved from https://www.jus.uio.no/lm/en/pdf/un.universal.declaration.of.human.rights.1948.portrait.letter.pdf
United Nations (1976) United Nations . (1976). International covenant on civil and political rights 1966. Retrieved from https://treaties.un.org/doc/publication/unts/volume%20999/volume-999-i-14668-english.pdf
United Nations (1989) United Nations . (1989). Convention on the rights of the child. New York, NY: UN. Retrieved from https://downloads.unicef.org.uk/wp-content/uploads/2010/05/UNCRC_united_nations_convention_on_the_rights_of_the_child.pdf?_ga=2.209651665.274437633.1540996300-199092997.1540996300
United Nations (2015) United Nations . (2015). Universal declaration of human rights. Illustrated edition. Retrieved from http://www.un.org/en/udhrbook/pdf/udhr_booklet_en_web.pdf
United Nations Human Rights Office of the High Commissioner (OHCHR) (1959) United Nations Human Rights Office of the High Commissioner (OHCHR) . (1959). Declaration of the rights of the child. Retrieved from www.ohchr.org/EN/Issues/Education/Training/Compilation/Pages/1DeclarationoftheRightsoftheChild(1959).aspx
United Nations Human Rights: Office of the High Commissioner (OHCHR) (1966) United Nations Human Rights: Office of the High Commissioner (OHCHR) . (1976). International covenant on economic, social and cultural rights. Retrieved from https://www.ohchr.org/en/professionalinterest/pages/cescr.aspx
Walt & Gilson (1994) Walt, G. , & Gilson, L. (1994). Reforming the health sector in developing countries. The central role of policy analysis. Health Policy and Planning, 9(4), 353–370.
World Health Organization (1946) World Health Organization . (1946). Constitution of the World Health Organization. New York, NY: WHO. Retrieved from https://www.loc.gov/law/help/us-treaties/bevans/m-ust000004-0119.pdf
World Health Organization (1978) World Health Organization . (1978, September 6–12). Declaration of Alma-Ata. International conference on primary health care. Alma-Ata, USSR. Geneva: WHO. Retrieved from http://www.who.int/publications/almaata_declaration_en.pdf
World health Organization (2015) World health Organization . (2015). Children’s rights in primary health care series. Retrieved from http://www.euro.who.int/en/health-topics/Life-stages/child-and-adolescent-health/publications/2015/childrens-rights-in-primary-health-care-series
World Health Organization Regional Office for Europe (2008) World Health Organization Regional Office for Europe . (2008). WHO European ministerial conference on health systems – Tallinn Charter: Heath systems for health and wealth. Tallinn: WHO.
Zdunek, Schröder-Bäck, Alexander, Rigby, & Blair (in press) Zdunek, K. , Schröder-Bäck, P. , Rigby, M. , & Blair, M. (2017). Report on the contextual determinants of child health policy. Available from http://www.childhealthservicemodels.eu/wp-content/uploads/Context-Culture-Report.pdf
- Prelims
- Chapter 1 The MOCHA Project: Origins, Approach and Methods
- Chapter 2 Models of Primary Care and Appraisal Frameworks
- Chapter 3 Listening to Young People
- Chapter 4 Child Centricity and Children’s Rights
- Chapter 5 Equity
- Chapter 6 The Limited Inclusion of Children in Health and Health-related Policy
- Chapter 7 The Invisibility of Children in Data Systems
- Chapter 8 The Conundrum of Measuring Children’s Primary Health Care
- Chapter 9 Measurement Conundrums: Explaining Child Health Population Outcomes in MOCHA Countries
- Chapter 10 Services and Boundary Negotiations for Children with Complex Care Needs in Europe
- Chapter 11 School Health Services
- Chapter 12 Primary Care for Adolescents
- Chapter 13 Workforce and Professional Education
- Chapter 14 e-Health as the Enabler of Primary Care for Children
- Chapter 15 Affiliate Contributors to Primary Care for Children
- Chapter 16 The Transferability of Primary Child Healthcare Systems
- Chapter 17 National and Public Cultures as Determinants of Health Policy and Production
- Chapter 18 Bringing MOCHA Lessons to Your Service
- Chapter 19 Evidence to Achieve an Optimal Model for Children’s Health in Europe
- Appendix 1: List of MOCHA Scientists
- Appendix 2: List of MOCHA Country Agents
- Index