
Listening to Young People
Issues and Opportunities in Primary Health Care for Children in Europe
ISBN: 978-1-78973-354-9, eISBN: 978-1-78973-351-8
Publication date: 6 May 2019
Abstract
Children’s voices are seldom heard directly. Most often, children, particularly young children, are represented by adults acting on their behalf who may or may not best represent the child’s views or best interests. This can be beneficial or problematic, if the child’s needs are not appreciated or recognised. This chapter looks at the changing attitudes to listening to young people, and the growing recognition of the value of children’s needs, as well as the growing voices of the children themselves, who make their needs increasingly clear. The results of our Models of Child Health Appraised (MOCHA) interviews with children and young people via the DIPEx International organisation give us clear direction as to the importance children using primary care services place on being taken seriously, being listened to and being able to make their own decisions. Other researchers asked input from primary care professionals on children’s autonomy and how the current and future primary care systems can best address the needs of young people, as well as the placing of these issues in a wider cultural context, and how this influences and is influenced by children’s choices. Finally, we look at how the MOCHA country agents have reported the assessment of the importance and function of listening to young people in our research.
Keywords
Citation
Zdunek, K., Alma, M., van Til, J., Groothuis-Oudshoorn, K., Boere-Boonekamp, M. and Alexander, D. (2019), "Listening to Young People", Blair, M., Rigby, M. and Alexander, D. (Ed.) Issues and Opportunities in Primary Health Care for Children in Europe, Emerald Publishing Limited, Leeds, pp. 55-76. https://doi.org/10.1108/978-1-78973-351-820191008
Publisher
:Emerald Publishing Limited
Copyright © 2019 European Commission
License
This chapter is published under the Creative Commons Attribution (CC BY 4.0) licence. Anyone may reproduce, distribute, translate and create derivative works of this chapter (for both commercial and non-commercial purposes), subject to full attribution to the original publication and authors. The full terms of this licence may be seen at http://creativecommons.org/licences/by/4.0/legalcode
Introduction
Listening to users, and adjusting services to make them relevant, attractive and accessible, is important in any dimension of health care. With children, this is equally important, as in this life period, health issues are best detected and addressed early, and salutogenic behaviour established, but of course listening to children does have practical and ethic challenges (Roth-Cline & Nelson, 2013). However, as demonstrated by the various approaches developed during the Models of Child Health Appraised (MOCHA) project, these challenges can be overcome successfully and fruitfully.
In this chapter, we look at the importance of listening to children and young people. Child centricity is an important tenet of the MOCHA project (see Chapter 4), and as part of this, we have tried to ensure that we not only have explored how children’s experiences, views and needs are taken into account of in the appraisal of primary care services for them in Europe, but also investigated how children’s experiences are taken into account, or influence the way primary care policy and services evolve in European Union (EU) and European Economic Area (EEA) countries. Sometimes, this is problematic, for example, children from marginalised populations (see Chapter 5) are poorly listened to or represented. The MOCHA project has investigated how the changing attitudes to children and young people have (or haven’t) shaped primary care services, what young people are saying about their care and the service primary care provides, what the public believe to be the case about care for children and societal reactions to child-centred issues that influence or change policy-making. Finally, in an exploration of the MOCHA results, we identify where there is disconnect between what children need and what is in place in the primary care systems of the EU and the EEA countries (see also Chapters 19 and 20).
Changing Attitudes to Listening to Young People
A fundamental premise of the MOCHA project is that of respecting the needs and rights of children as a unique population group (see Chapter 4). We committed to being child-focussed and child-centric, with services being designed to meet need. In this context, we sought to identify what constitutes optimal care for children in primary care services and to find means by which this can be achieved by the different primary care services in Europe. This cannot be achieved without seeking the views of young people themselves.
Children are far more than ‘adults in waiting’, but have specific health needs and requirements of the primary care health services. We have seen, in the process of the MOCHA project, that children are often required to mould their needs of health care into a structure that is exclusively adult-focused and adult-designed. In addition, research into children’s health and health services is more often than not an exercise in navigating systems and structures that are not designed with children in mind, and even basic statistics on services for children and their outcomes are hard to obtain (see Chapters 6 and 7).
As described in Chapter 4, the perception of ‘what is a child’ has changed, resulting in today’s concept of child empowerment, not as a mini adult, but as a distinct individual with specific needs. This has resulted in the recognition that there is a need to define and respect a child’s health and role in the health services (Rosa & Matysiuk, 2013). Current thinking on child rights acknowledges that children’s views and rights are recognised by the United Nations (UN) and almost all UN member states including all EU and EEA nations (UNHCR, 2018) and by the World Health Organization as a fundamental tenet of health, ensuring their healthy growth and development ought to be a prime concern of all societies (Chapters 2 and 4; WHO, 2018).
Such a change can be seen as a shift in socio-cultural perceptions of the child as having intrinsic, rather than extrinsic value, and this is explored in more detail in Chapters 4 and 17 of this report. Culture in this sense can be defined as the results of material and ideas-based concepts. Values and accepted ways of doing things are adopted and objectified by groups of individuals, transferred to other groups and to the next generations (Szczepański, 1963). It is this process that creates societal attitudes towards children and the value that we place on them. This was reflected in health policy analysis, which has developed to seek to understand the actors involved, including children (see Chapter 1). This approach to policy-making and enabling children via their agents (see Chapter 4), to contribute to policies that affect them can be seen as a cultural change. It is one that allows deep insight into the analysis of primary care for children and is one that MOCHA has adopted.
In the MOCHA project, through analysis of national information received from the MOCHA country agents (see Chapter 1) and from other research activity, increasing focus on the child as a central actor in policy-making has been identified. We found that children are often the main object (directly and indirectly) of debates and discussions related to child primary health care across most of the European countries (Blair, Rigby, & Alexander, 2017; Zdunek, Schröder-Bäck, Blair, Rigby, 2017). This focus can take many forms, such as the child as an object of policy decisions:
as a well-child embedded in a family context and a broadly understood social environment or preventive care context; and
the child with long-term illnesses and/or complex health care needs at the centre of the debate.
Although the child is not usually an active participant in policy creation or shaping, he or she becomes a causative actor in the process, because they are the subject of the policy. As described in Chapter 4, the child is surrounded by a range of representatives – who either have a direct influence on the child (as part of the family or immediate social environment –including teachers, neighbours, family physicians and nurses), or an indirect and more distant involvement (including professional groups, health care practitioners representing the health care system, government representatives and the media). At present, changing attitudes to the child have resulted in a number of influences on child health policy, including the child and proximal and distal agents of representation.
Incorporating Young People’s Views and Experiences
It is particularly important, when thinking about a child’s experience of primary health care, to listen to what children need and understand what they expect and experience from primary care services. Children’s lack of autonomy and power means they have very little opportunity to effect change or influence how care is delivered to them. By assessing a child’s experience of the health care service, this provides important evidence about the best way to run and provide services.
Including the views of children, young people and their parents are essential components in the appraisal of primary health care for children in Europe. This needs to be proactive and planned, since children do not complete surveys, fill out comments cards or make complaints. Parents, particularly of younger children, or parents faced with newly arising health problems in their child, may not want to antagonise the health professionals and system with which they are dealing and may not know what service norm to expect. It is necessary to actively seek such views.
DIPEx: Qualitative Inquiry into Children’s Experiences
Qualitative inquiry into children’s and parent’s experiences of primary health care for children provided valuable triangulation of results and identification of areas of concern for children, young people and their families. Qualitative researchers from institutions in five different countries that are part of the DIPEx International network (www.dipexinternational.org) worked collaboratively to explore children’s experiences of primary care in their respective countries across Europe: Czech Republic, Germany, The Netherlands, Spain and the United Kingdom. These were the only EU/EEA countries with a DIPEx member, but this list included a representative sample of different types of primary care system. The specific objective of this task was to provide insights into the experiences of children and parents in terms of primary health care for children.
Data Collection
The qualitative research methodology used by the MOCHA project was developed by the Health Experiences Research Group (HERG) University of Oxford (Ziebland & Herxheimer, 2008). This methodology includes narrative and semi-structured interviews. The relatively unstructured, open-ended nature of the interview method helps to identify participants’ own concerns, meanings and priorities rather than being led by a highly focused research interest (Riessman, 2008). We focused on the experiences of children as well as their parents. Participants were recruited using maximum variation sampling, which involves including a broad range of experiences and demographic characteristics (Coyne, 1997; Marshall, 1996). We aimed to identify and include the widest range of experiences of children and parents in terms of primary care services for children, rather than to identify the numerical distribution that exists in the wider population. We focused on the experiences of ‘healthy’ children, children with (complex) mental health conditions and children with (complex) physical health conditions and their parents. In total, 84 children participated in the study.
Data collection consisted of in-depth interviews, focus group interviews and a secondary analysis of interviews conducted in earlier studies in one of the five countries. Interviews and focus group discussions were analysed for themes that structured participants’ experiences using a thematic analysis combined with constant comparison. Table 3.1 gives an overview of the number of children that participated in the study per country.
Overview of number of children and number and type of interviews in each country.
| Total | Czech Republic | Germany | Netherlands | Spain | UK | |
|---|---|---|---|---|---|---|
| # in-depth interviews | 38 | 13 | 1 | 7 | 6 | 11 |
| # focus group interviewsa | 5 (26) | 1 (5) | 2 (14) | – | 1 (3) | 1 (4) |
| # secondary analysis interviews | 20 | – | 14 | – | – | 6 |
Note: aIn brackets number of participants of the focus group interview.
Communication and Relationships with Health Care Professionals
The complete findings of this research can be found in Alma, Mahtani, Palant, Klůzová Kráčmarová, and Prinjha (2017) which discusses in detail the issues that are important to children, young people and their families. Examples of these issues are described here, including communication and relationships with primary care and the importance of involvement and participation in care. Communication and relationships with health care professionals play pivotal role for children in terms of what is good about primary care and what they felt needs to be improved. Communication and relationships were reported as a key quality component. Issues about communication skills, positive attitude towards the child and parents, a trustful relationship and professionalism were the main aspects valued by the participants. Openness to discussion, communication and taking into account the child’s opinions about treatment were seen as a sign the child is respected by the health care professional. Other communications skills that were valued were being empathetic, easy to talk to and really listening to what the child or parent is saying.
What I think they should do – they should, they should be relaxed. I know being a doctor’s really stressful and it’s very […] well I don’t know that, I don’t know why I’m saying that. But I know it can be stressful because of having a job like that is stressful. But I feel like they should be […] they should relax themselves, should be relaxed. They should interact, they should […] because if you, if you just […] if you tone it down […] if you tone down your, if you tone down the professionalism to some extent and to more of a social […] to more of a […] to more of an informal sort of stance, then it would definitely have […] it will definitely […] you’ll definitely engage with teenagers that way. Because teenagers don’t like formality, and I feel like it’s important to engage with teenagers and so it’ll be a bit more […] to be a bit more chilled. (UK, M, child)
Children stressed also the importance of building a trusting relationship with their health care professional. In order to be able to build such a relationship, children stressed the importance of seeing the same professional every time. Meeting with the same health care professional helps young people to have relaxed conversations, feel at ease and build a relationship.
I think it is better to see the same doctor every time, especially the same GP. Because I know, the doctors ask you about your medical history every time. And then you do not have to tell them the same things all over again. (G, F, child)
Although seeing the same doctor every time was important to almost all participants, many recalled seeing different professionals every time they visited the doctor. Many children perceived a lack of continuity of care. This resulted in distress, as children met new people each time and had to repeat their story to different health care professionals as a result. A lack of coordination in primary care systems was perceived by several participants. This can have serious consequences for children, particularly for a child with complex long-term conditions.
Involvement and Participation in Care
Children and young people felt that they should be involved in managing their own care. They varied in how much parental involvement they desired and if they prefer to visit a primary health care professional alone or with their parents. Many children we interviewed said they visited primary health care services with their parents. Factors influencing the decision to visit the general practitioner alone or with someone else included: age, the reason for the visit, level of control by the parents, accessibility and transport. The disadvantages of visiting health care professionals with parents were discussed.
Another key point identified was that of being part of the conversation. Several children recalled that the doctor often spoke to the adult rather than to the child, which they found annoying.
I can remember thinking I hope this goes away but also that I was slightly annoyed that they had not paid any attention on mine to what I’d been saying. (UK, M, child)
So I think the GP, or the health professional in general, should really just ask the young people what they feel like they need. (UK, F, child)
For successful participation of children in health care, it is important that children’s contributions are taken into account and acted upon (Schalkers, Dedding, & Bunders, 2014). However, decisions are often made in cooperation with parents.
I think the doctors should speak more with the child. […] I don’t know why they cannot ask the child directly. When I am ill and I go to the doctor, I lie down, the doctor examine me, leave me lying there and then he speaks with my father about everything. ‘Since when does she feel sick?’ and I could be sick earlier, I just didn’t say that at home, right? And I think it is wrong, they should talk to the child who is sick […]. (CZ, F, child)
A number of other issues that are important to children and young people were identified in this qualitative study: accessing primary care services, physical environment of the primary care facility, role of schools, financial issues and medical records. These are fully discussed in Alma et al. (2017).
Parent’s Opinions and Experiences on Children’s Autonomy
In addition to gathering the views of a group of children, the MOCHA project also sought public views on primary care services and how they address the needs of children. This gave us the views of adults on behalf of children they represent. The report: Public Priorities for Primary Care for Children. A report on public preferences for patient-centred and prevention oriented primary child health care models for children (van Til, Groothuis-Oudshoorn, & Boere-Boonekamp, 2018) aimed to elicit formative values from the general public in five European countries and determine public priorities in the assessment of the quality of a child-oriented primary care system. This was a descriptive, cross-sectional, quantitative study of a representative sample of the general public in five European countries (Germany, the Netherlands, Poland, Spain and the United Kingdom). We sought the public’s experiences and perceptions of the quality of the currently provided primary care for children, particularly with respect to the children’s primary care. We developed the Preferences for Child Health Care Assessed (POCHA) questionnaire as a research instrument, which was translated into Dutch, German, Polish and Spanish (van Til et al., 2018).
In accordance with the children’s need for good communication, good access and the need for trust and respect from their primary care providers, one of the foci of the POCHA questionnaire was autonomy of children. This relates in particular to the attributes of quality of care in terms of accessibility, confidentiality and empowerment.
In total, 2,403 adult respondents filled out the POCHA questionnaire. To be able to analyse specifically the opinions and experiences of parents about child autonomy, the respondents who are parents of a child or children aged under 18 years (N = 872) were selected. This resulted in 143 respondents from Germany (DE), 148 from the Netherlands (NL), 173 from Poland (PL), 235 from Spain (ES) and 173 from the United Kingdom (UK).
The results presented in this chapter are based on the topics of what parents consider to be desirable with respect to children’s autonomy (10 questions) and what parents have experienced with respect to children’s autonomy (nine statements).
Opinions
In the beginning of the POCHA questionnaire, we asked respondents with children aged under 18 years: ‘Can you tell us at what age you think a child should be able to do the following?’ for ten items related to autonomy.
The overall opinion of respondents of the five countries on the age a child ‘should be able to do’ the items is presented in Figure 3.1. For all ten autonomy items, the age of 16 years seems to be an important marker to respondents. The figure also shows that respondents think differently about the different items, for example they feel that a child should know about the range of services at a much younger age (89% said at least at the age of 16 years) than that a child should be able to limit access to his or her medical records from his or her parents, in order to protect privacy (43% said at least at the age of 16 years).

In order to study how the five countries relate to each other in terms of the overall opinion on autonomy of children, the respondents’ answers on the ten questions were averaged. Figure 3.2 shows that respondents from the Netherlands and Germany assign autonomy to children at a younger age than, for example, respondents from Spain or Poland.

As the age of 16 years seems to be an important marker to respondents, we analysed whether countries differ in opinion on what a child should be able to do first. The five countries’ respondents agreed that knowing about the range of services available in health care and how to access them is the item a child should be able to do first. They also agreed on the item that a child should be able to do the latest: namely limiting access to his medical records from his parents. However, agreement on this item ranges a lot; 23.7% of respondents in Poland agree that a child should be able to do this at age 16 compared to 62.4% in the United Kingdom.
Experiences
In the POCHA questionnaire, we also asked respondents with children under 18 years of age about the experiences they have had with primary care for children in their country. Each participant was presented with statements about potential quality of primary care for children and was asked to indicate to what extent he/she agreed or disagreed. We used a scale of ‘strongly disagree’ to ‘strongly agree’. Again, this exercise was designed to measure the experiences of parents about child autonomy. Therefore, we selected the nine items related to accessibility, confidentiality and empowerment to illustrate this.
The results are presented in Table 3.2 and visualised in Figure 3.3.
Percentage of agreement (summed percentage of respondents that agree and strongly agree) with the statements on autonomy-related attribute items, indicated by the respondents of the five countries.
| Statements | % Agreement with Statement, Per Country* | Pearson χ2 | p-value | |||||
|---|---|---|---|---|---|---|---|---|
| DE | NL | PL | ES | UK | Average | |||
| Children and/or their parents can make an appointment with other primary care providers without a referral from the main primary care provider (accessibility) | 69.0 | 56.4 | 36.1 | 50.9 | 58.8 | 53.8 | 30.6 | 0.015 |
| Children and/or their parents can make an appointment with secondary or other health care providers without a referral from a primary care provider (accessibility) | 64.9 | 69.0 | 65.2 | 57.4 | 40.5 | 59.0 | 19.0 | 0.268 |
| Children and/or their parents know about the range of services available in primary care and how they can access them (accessibility) | 52.9 | 72.7 | 74.4 | 64.2 | 84.4 | 73.1 | 22.7 | 0.119 |
| A child and/or his parents have access to a child’s medical records (accessibility) | 65.4 | 88.0 | 80.5 | 59.7 | 75.9 | 70.8 | 32.1 | 0.010 |
| A child has the right to a confidential consultation with the primary care provider (confidentiality) | 80.0 | 75.0 | 37.8 | 52.4 | 66.7 | 60.8 | 39.1 | 0.001 |
| In primary care, a child can limit their parents’ access to the child’s medical records in order to protect his privacy (confidentiality) | 29.4 | 48.7 | 11.6 | 33.3 | 41.5 | 32.7 | 30.7 | 0.014 |
| In primary care, the child and/or the parents have to authorise other health care providers accessing the child’s medical records (confidentiality) | 68.1 | 64.1 | 86.1 | 47.4 | 49.0 | 66.0 | 12.5 | 0.706 |
| In primary care, a child can express his opinions about his health management independently from his parents (empowerment) | 60.7 | 63.9 | 40.5 | 41.4 | 63.4 | 52.5 | 28.2 | 0.030 |
| In primary care, children and/or their parents are involved in decisions about the management of the child’s health (empowerment) | 85.2 | 68.6 | 67.9 | 61.4 | 93.6 | 74.0 | 35.8 | 0.003 |
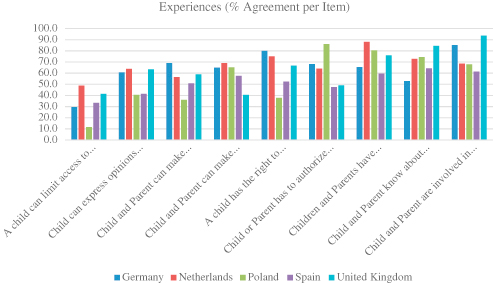
Accessibility
Respondents’ experiences show that improvements with regard to accessibility are achievable. More than half of respondents (53.8%; range 36.1% for Poland to 69% for Germany) agree that children and/or their parents can make an appointment with other primary care providers without a referral from the main primary care provider; percentages are slightly higher for making an appointment with secondary or other health care providers (59.0%; range 40.5% for the UK to 69% for the Netherlands). Almost three-quarters of respondents agree that children and/or their parents (73.1%; range 52.9% for Germany to 84.4% for the UK) are well informed about the range of services available in primary care and how they can access them. More than two-thirds of respondents (70.8%; range 59.7% for Spain to 88.0% for the Netherlands) have the experience that their child and/or they themselves have access to the child’s medical record.
Confidentiality
With respect to confidentiality items, 60.8% (range 37.8% for Poland to 80% for Germany) confirms that a child has the right to a confidential consultation with his primary care provider. Only 32.7% (range 11.6% for Poland to 48.7% for Germany) of respondents agree that in primary care a child can limit parental access to the child’s medical records in order to protect his privacy. About two-thirds (66.0%; range 47.4% for Spain to 86.1% for Poland) confirm that the child and/or the parents have to authorise other health care providers accessing the record.
Empowerment
Respondents’ experiences related to empowerment items are diverse. More than half of respondents (52.5%; range 40.5% for Poland to 63.9% for the Netherlands) answer that a child can express his opinions about his health management independently from those of the parents. almost three-quarters (74%; range 61.4% for Spain to 93.6% for the UK) agree that in primary care, children and/or their parents are involved in decisions about the management of the child’s health.
Societal Reactions
The context of child primary care is not just placed with the users and providers, but is inextricably linked with the wider cultural context (see also Chapters 4 and 17). As part of the MOCHA project, we investigated the effect of societal reactions to issues that affect children. We looked at particularly sensitive national concerns and how they affected popular perceptions of what child primary care should be for and how it is run in countries (Zdunek, Schröder-Bäck, Blair, Rigby, 2017). The MOCHA country agents identified two or three recent societal debates in their country, which involved children’s health and well-being. They described wide variety of cases, demonstrating the broad perspectives of children’s health and health services. Many of the issues described were very different, but all had certain elements in common. Essentially, the concerns in Europe about children’s health are twofold. On the one hand, attention was given to issues relating to organisational factors of the care of children, involving those indirectly concerned with children as patients; on the other hand, some issues directly involved children themselves, such as cases of child abuse, care of children in hospital, childhood obesity, homelessness or poverty (Zdunek, Schröder-Bäck, Blair, Rigby, 2017). Children are seen in two broad domains – either that of the generally healthy child embedded in a family context, where attention is focused on preventive actions, or as a sick child, or a child with a long-term condition, who has need of specific attention from the health services.
Child health issues can be particularly sensitive and thus can provoke strong societal reactions that may eventually shape national health policy. Public voices can stimulate policy change, when a government is reluctant or unable to deliver because of lack of political interest, inflexible public administrations, resource constraints or lack of trust in certain populations (Greer, Kosińska, & Wismar, 2017). Civic society, in the form of informal movements or public discussions, brings expertise, ideas and diverse perspectives to the field of health policy-making, particularly child health policy-making. Indeed, the effectiveness of child health policy initiatives increases the more there is involvement of relevant actors.
The means by which the public express their dismay or support of an initiative or system change can also support or hinder the process of policy development (see also Chapter 17). In addition, public expression can also stimulate change without appropriately informed debate as to the intended or unintended consequences of the resulting action. In MOCHA, we investigated the vehicles of public expression, to characterise how the public sentiment was raised and continued.
In the research process, we were able to identify four distinct areas of public expression: actors, actions, communication and information. Actors who were directly involved in the process of children’s health care, such as parents and individuals, politicians and academics, experts and stakeholders and non-governmental organisations (NGOs), expressed opinions through actions such as protests and strikes, campaigns, debates and petitions, social media activity or emotional reactions. Additionally, they were often supported by philanthropic and political initiatives. Public attention was maintained through various communication channels, most commonly social media, traditional media and the internet. Information is becoming more readily available, via official government internet websites, social media or other channels, such as articles in the press, documentaries and educational films, as well as publications of reports, which help to keep the issue in the public eye. Those elements supplement each other and therefore they cannot be analysed separately
Actors
Expression of the process of policy change or the desire for change is manifested by certain actors, including those representing children in the proximal and distal sense (see Chapter 4). These could be individuals such as children, parents or journalists, or organisations such as political parties or NGOs. For instance, childhood obesity in Malta was highlighted as an issue and an object of policy campaigning by politicians and academics in the country, and political debates in Finland and the United Kingdom were held about the services and treatment given to unaccompanied child asylum-seekers.
In Ireland, objections to changes in the Discretionary Medical Card (which enables health care free of charge) were voiced by a range of actors who inspired much public support. These actors organised a strong social media campaign and online petition to the government and were supported by public support foundations and NGOs. These actors aimed to reverse a decision that many felt resulted in inequity of (lack of) provision to vulnerable children. In Romania, the inappropriate treatment and overmedication of children in residential children’s home was exposed by journalists as actors representing the rights and needs of the children.
A private foundation (Paracelsus NGO) advocated ‘freedom of choice’ by publicising an anti-vaccination rhetoric in the media in the Czech Republic, against the mandatory vaccination policy of that country. There has also been much debate in Italy, where compulsory vaccination has recently been revoked due to the influence of anti-vaccination sentiments.
Public expression can take place by the actors directly involved, or opinions are expressed through actions, such as a strike (as was the case in Poland), or a vigil (such as that held by parents protesting at changes to eligibility for Discretionary Medical cards).
Actions
Actions such as public protests, strikes, campaigns, debates and petitions are common societal reactions to issues that are perceived to affect children unjustly. Examples of this have been reported in relation to issues pertinent to children in Greece, Italy, Ireland Lithuania and Norway (Blair et al., 2017) among other countries. In Croatia, there were public protests related to mandatory vaccination, disabled children’s rights and child abuse. In Poland, the nurses went on strike in protest at poor remuneration and stressful working conditions, which were supported by patients and nurses from health centres other than the hospital where the protest initiated. The nurses’ strike was also met by protests by groups of parents who argued that they should find another means of expressing their discontent, as their actions risked harming children further in their eyes.
Another form of action is the creation of a petition, which is a demonstration of the depth of support for an issue. In France, there was a public protest against the DTP vaccination, an action that began with a petition which eventually collected over one million signatures. In the Czech Republic in 2010, a group of parents presented a petition against mandatory vaccination. A petition was also created in the Czech Republic to express disquiet about the need to unify services, despite the fact that concern had been previously raised about the fragmentation of services and the complex system. In Ireland, a petition was organised by those objecting to the decision to build a national children’s hospital in the centre of Dublin. Social media and Web-based campaigns resulted in over 60,000 signatures.
Media campaigns are another common action that has been used to increase public awareness about an issue. In Ireland, the issue of homelessness was discussed nationally after being highlighted in a television programme, and within the UK, and in Northern Ireland, child sexual exploitation was exposed in this way.
Philanthropic actions can also be seen as a form of societal reaction to national situations. The presence of food banks in Spain is one such example as a reaction to the hardship felt by many families. In Norway, the scandal of a young boy who was a victim of child abuse led to members of the public leaving flowers at the entrance to the hospital where he was treated. Emotional actions, similarly, are often used to support and stimulate the retention of an issue in the public psyche. In Poland, for example, support for and resistance to the nurses’ strike was maintained by stressing the emotional aspects of events that led to the strike. This was characterised by presenting the children as innocent victims of a ‘heartless system’, ‘insensitivity of officials’, ‘nurses concerned only with money’, and ‘political manipulation’. Politicians were also seen to use emotional pressure on the striking nurses, and the opposition politicians accused the government of disinterest in the fate of nurses and their patients.
Communication
For any protest or reaction to be successful, communication is essential. The means of this is changing, relying increasingly on social media rather than official methods such as printed media or television. Social media, in particular, is increasingly powerful as it functions to support campaigns. Electronic communication played a crucial role in almost all cases described by the MOCHA country agents.
Shocking events were almost always reported in the media – such as news, newspapers, online and so on, and these provoked a national discussion. This allowed the actors, such as parents and other stakeholders, to speak publicly about their issues.
For example, in Croatia, a parent witnessed child abuse by an employee at the Croatian ‘Special Hospital for Protection of Children with Neurodevelopmental and Motor Disorders’. This was shared through social media, which caused a scandal and resulting heavy coverage by the national media. An explanation and disciplinary action were demanded by the public as a result. In the United Kingdom, the news and social media were instrumental in raising concerns about immigration and facilitating actions. Images and stories were shared regularly and societal actions resulted. These ranged from a public march to welcome refugees, which saw thousands congregate to support asylum-seekers and refugees in September 2016, to petitions that oppose refugees and asylum-seekers entering the United Kingdom.
New regulations on nutrition for young people sparked social media protests in Poland. High school students claimed that they wanted to decide on their own diet, resulting in a petition and discussion among young people, parents, politicians and businesses.
Traditional media, such as newspapers, television and radio remain a key aspect of societal reactions to policy changes. Public debates are sustained through Web-based initiatives and traditional press. Awareness of childhood obesity was raised in Austria through daily newspapers, televisions and other campaigns. They often used attention-grabbing headlines such as ‘Each fifth child is overweight’ or ‘the fight against obesity’, ‘Our children grow ever fatter’.
Information
Without information, societal reactions do not happen. What is an issue is whether the information is reliable and truthful. Information is shared by active actors, through various communication channels. National and local news reports are instrumental in raising many types of concerns, and as a result, public opinion and trends can have a significant impact on decisions about health systems. For example, an Irish television documentary called ‘My Homeless Family’ about the experiences of homeless families and those living in emergency accommodation was televised a month before a general election. This, combined with wider debate and emerging statistics about the increase in homelessness in Ireland, turned it into an election issue. This was also informed by a report entitled Homeless Truths (Ombudsman for Children’s Office, 2012), which described children’s experiences of homelessness; simultaneously, the Ombudsman for Children also launched a series of recordings of the young people’s interviews that were used in the study. In Latvia, educational films about bullying in schools and cyberbullying were created from national reports and research, to respond to increasing concerns about bullying. The goal of these films was to provide information to empower pupils and teachers to understand and deal with bullying, its nature and consequences. The Association of Hungarian primary care paediatricians produced publications outlining the issue of unclear health certificates for children attending summer camps in Hungary; in the United Kingdom, charities and other organisations produced reports on the challenges faced by unaccompanied asylum-seeking children and called upon the government to do more to help them.
The childhood obesity debate in the United Kingdom, particularly in Scotland, was fuelled by a number of reports published by the Scottish Government on the health and economic burden of obesity in Scotland in 2015. Targets were subsequently set to reduce the prevalence of obesity, and a ban on advertising junk food was extended in the country.
Environmental pollution was a topic of discussion in Italy, after a number of press articles and the Higher Institute of Health report known as the ISTISAN Report. The data in this report were published on the website of the Higher Institute of Health and refer to a study commissioned by the Ministry of Health to implement prevention strategies after increased mortality and hospitalisation had occurred in an area where considerable amount of waste was incinerated (Blair et al., 2017)
MOCHA Country Agent Questions about Children
In addition to independent research in MOCHA to listen to children and young people, or to gain the views of their representatives, we also asked the country agents to identify policies and practices in their countries that facilitated or restricted children from giving their views or influenced health services for young people. The country agents were not able to obtain views of children themselves, because of ethical permissions, nor were they able to give opinions about their country. However, they were able to provide examples and instances of where each country was particularly child-friendly, or which countries made it more difficult for children to participate and collaborate in their own primary care.
Within 40 sets of questions to the country agents, all of which were child-focused in some way; 15 directly investigated children’s experiences. Subjects that were subject to MOCHA’s attention were migrant and refugee children, long-term complex conditions, chronic physical and mental conditions; vulnerable children (e.g. those in the care system); children’s corporate autonomy and how well this is catered for in each country; the use and regulation of health apps and helplines; and home-based records where parents and children can have access and input.
Equity of Provision for Young People
MOCHA country agents answered questions about equity of provision for two particularly vulnerable groups of individuals, refugee and asylum-seeking children and children living in out of home societal care (foster or residential care). These child populations can be seen as representative of the equity of provision in primary health care in their countries, more about which is discussed in Chapter 7. The country agents were asked to provide policy references, about whether these children received the same health care as other children in their country and whether they received less care or particularly targeted care – which may or may not result in intended or unintended consequences.
Children with Complex Care Needs in the Community
Country agents identified particular points of care for children living with complex care needs. Tracer conditions chosen to represent this group of vulnerable individuals were those on long-term ventilation, those with traumatic brain injury and those with intractable epilepsy. In order to establish the primary care and community support that children and families had in their countries, country agents identified the different agencies involved in every day care, the extent to which families and children are consulted and input into their care plans, and the ease at which good quality and relevant support could be obtained and sustained.
Children with Long-term Mental Health Needs in the Community
Country agents were tasked with identifying the level of support and care children with long-term mental health needs experience in primary care and the community. Tracer conditions of Autism and ADHD were used to represent all children with complex needs, as the management and treatment of these are typical of many other forms of mental health care. Issues such as the policy around access to education support for children and families and the extent to which they can access and input into their care were explored by the country agents.
Social Care and Child Protection
Children who are in need of social care support, and how this links to primary care services in the community, were investigated by country agents, by extending one of the vignettes developed to describe a child with complex care needs, in this case, a traumatic brain injury. This allowed the country agents to explore the relationship between social care needs and health care needs and how easy it is for children and families to access the correct levels of support. Child protection is an important element of this, and we wished to know if policy allowed easy access to services in a case of vulnerability; the issue of child protection was also investigated in terms of children in foster care and equity (see Chapter 7).
Children with a Long-term (Chronic) Condition
Asthma was the main tracer condition used to identify the extent to which children can self-manage any long-term conditions. The country agents identified areas in which children were able, or not, to manage their own medication (such as in school), access transition from children’s services to adult services, and the extent to which policy allows adolescents can seek advice independently and make their own decisions about their care.
Autonomy of Choice
We asked about whether policy allowed children to independently access care, such as in the case of reproductive health or contraception, health advice and education or treatment – or whether the system did not facilitate this without parental or guardian knowledge or payment. The country agents also investigated whether children could override parental decisions about their health, such as in the case of vaccinations.
Use of Apps, Websites and Helplines
Country agents explored the information that is most accessible and attractive to children and young people, namely, that contained in apps, websites and helplines. The extent to which these are regulated for accuracy of advice in each country and the types of data that are collected by the sites were investigated by the country agents.
Home-based Records of Children’s Health
We asked about home-based records, the range of their use, means of extending them to children moving into a country and the extent to which parents and older children can contribute to the types of data they collect and whether they can independently record data that will subsequently be used to improve and coordinate services. For more information, see the full report by Deshpande, Rigby, Alexander, and Blair (2018).
Summary
Listening to the views of children and young people is essential in designing and appraising primary care systems to serve them. However, listening is not necessarily an easy task. Children are often necessarily represented by others, which can be beneficial or increase their vulnerability. When the opinions of those representing children are taken into account, care must be taken that they represent their best interests. Research in this area is challenging, but at the same time, vitally important.
The DIPEx findings show that although many children were satisfied with the primary health care services for children, it is not a universally good picture. While some of the needs of the children, young people and their families are complex and beyond the influence of an individual health professional, other concerns are clearly within a health care professional’s ability to improve. Careful interpretation and analysis of patients’ subjective experiences highlighted what is working well in primary care services for children, what needs to be changed and how to go about making improvements (Alma et al., 2017).
Tips for health care professionals: try to pay sufficient attention to your patients, and if it is a child, try to explain him or her everything as clear as possible. If the child is older, please evaluate what the child already knows and anticipate. (NL, F, child)
Similarly, the POCHA questionnaire reflects, to a great extent, the perceptions stated by the children in the qualitative interviews about primary care carried out by the DIPEx group. What is interesting, however, is that in Poland and Spain, there seems to be less capacity or cultural acceptance of child autonomy in the management of their health than in Germany, the Netherlands and the United Kingdom (see also Chapter 17).
Indeed, recognising that children grow steadily in understanding, knowledge and the wish to be treated as individuals is a key issue throughout all the work reported in this chapter. It also comes to light in Chapter 10 about children with complex needs and enduring conditions, and in Chapter 14 about E-Health. The wider issues of the growing awareness and autonomy of the child are picked up further in Chapter 19.
In terms of societal reactions to the health care of children, it is clear that issues involving children are emotive and tend to readily provoke national debates. Predominantly, public concerns identified by the MOCHA country agents were directly or indirectly related to health care of children. Some issues became part of public awareness for only a few weeks, such as the national debate about contraception for adolescent girls in France, and others remain in the public consciousness for many years – such as the debates about compulsory vaccination in Italy or the proposed location of the national children’s hospital in Ireland. In the MOCHA project, we have tried to elucidate the views of children directly or via actors on their behalf as well as aiming to establish the extent to which children’s views are considered important in the policy environment and in the evolution of national primary care services.
References
Alma, Mahtani, Palant, Klůzová Kráčmarová, & Prinjha (2017) Alma, M. , Mahtani, V. , Palant, A. , Klůzová Kráčmarová, L. , & Prinjha, S. (2017). Report on patient experiences of primary care in 5 DIPEx countries. Retrieved from http://www.childhealthservicemodels.eu/publications/technical-reports/
Blair, Rigby, & Alexander (2017) Blair, M. , Rigby, M. , & Alexander, D. (2017). Final report on current models of primary care for children. Retrieved from www.childhealthservicemodels.eu/wp-content/uploads/2017/07/MOCHA-WP1-Deliverable-WP1-D6-Feb-2017-1.pdf
Coyne (1997) Coyne, I. T. (1997). Sampling in qualitative research. Purposeful and theoretical sampling: Merging or clear boundaries? Journal of Advanced Nursing, 26, 623–630.
Deshpande, Rigby, Alexander, & Blair (2018) Deshpande, S. , Rigby, M. , Alexander, D. , & Blair, M. (2018). Home based records. Retrieved from www.childhealthservicemodels.eu/wp-content/uploads/R15-Home-Based-Records-Report.pdf
European Parliament and European Council (2005) European Parliament and European Council . (2005). Directive 2005/36/EC of the European Parliament and of the council of 7 September 2005 on the recognition of professional qualifications. Official Journal of the European Union. L255/22, Article 31. Retrieved from https://eur-lex.europa.eu/LEXUriServ/LexUriServ.do?uri=OJ:L:2005:255:0022:0142:EN:PDF
European Parliament and European Council (2013) European Parliament and European Council . (2013). Directive 2013/55/EU of the European Parliament and of the council amending Directive 2005/36/EC on the recognition of professional qualifications and Regulation (EU) No 1024/2012 on administrative cooperation through the International Market Information System (‘the IMI Regulation’). Official Journal of the European Union. L 354/132. Retrieved from http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32013L0055&from=EN
Greer, Kosińska, & Wismar (2017) Greer, S. L. , Kosińska, M. , & Wismar, M. (2017). What is civil society and what can it do for health? In S. L. Greer , M. Kosińska , & M. Wismar (Eds.), Civil society and health, contributions and potential, European observatory on health systems and policies (p. 12). World Health Organization. Retrieved from www.euro.who.int/en/about-us/partners/observatory/publications/studies/civil-society-and-health-contributions-and-potential-2017
Marshall (1996) Marshall, M. N. (1996). Sampling for qualitative research. Family Practice, 13, 522–525.
Ombudsman for Children’s Office (2012) Ombudsman for Children’s Office . (2012). Homeless truths: Children’s experience of homelessness in Ireland. Retrieved from www.oco.ie/app/uploads/2017/09/HomelessTruthsWEB.pdf
Riessman (2008) Riessman, C. K. (2008). Narrative methods for the human sciences. Thousand Oaks, CA: Sage.
Rosa, & Matysiuk (2013) Rosa, R. , & Matysiuk, R. (2013). Ewolucja praw dziecka (aspekty filozoficzne, pedagogiczne i prawne). In E. Jagiełło, & E. Jówko (Eds.), Dziecko w kulturze współczesnego świata (pp. 10–33). Siedlce ISBN 978-83-936635-2-1. Retrieved from https://docplayer.pl/4327137-Dziecko-w-kulturze-wspolczesnego-swiata-redakcja-naukowa-ewa-jagiello-ewa-jowko.html
Roth-Cline & Nelson (2013) Roth-Cline, M. , & Nelson, R. M. (2013). Parental Permission and child assent in research on children. Yale Journal of Biology and Medicine, 86(3), 291–301.
Schalkers, Dedding, & Bunders (2014) Schalkers, I. , Dedding, C. H. M. , & Bunders, J. F. G. (2014). ‘[I would like] a place to be alone, other than the toilet’ – Children’s perspectives on paediatric hospital care in the Netherlands. Health Expectations, 18, 2066–2078.
Szczepański (1963) Szczepański, J. (1963). Elementarne pojęcia socjologii. Warszawa: PWN.
United Nations Human Rights Office of the High Commissioner (UNHCR) (2018) United Nations Human Rights Office of the High Commissioner (UNHCR) . (2018). Declaration of the rights of the child (1959). Retrieved from www.ohchr.org/EN/Issues/Education/Training/Compilation/Pages/1DeclarationoftheRightsoftheChild(1959).aspx
van Til, Groothuis-Oudshoorn, & Boere-Boonekamp (2018) van Til, J. , Groothuis-Oudshoorn, K. , & Boere-Boonekamp, M. (2018). Public priorities for primary care for children. Retrieved from www.childhealthservicemodels.eu/wp-content/uploads/member-files/Final-Report-POCHA_14-08-2018.pdf
World Health Organization (2018) World Health Organization . (2018). Child health. Retrieved from https://www.who.int/topics/child_health/en
Zdunek, Schröder-Bäck, Alexander, Rigby, & Blair (2018) Zdunek, K. , Schröder-Bäck, P. , Rigby, M. , & Blair, M. (2018). The culture of evidence-based practice in child health policy - A report. Retrieved from www.childhealthservicemodels.eu/wp-content/uploads/Evidence-Based-culture-Report.pdf
Zdunek, Schröder-Bäck, Rigby, & Blair (2017) Zdunek, K. , Schröder-Bäck, P. , Alexander, D. , Rigby, M. , & Blair, M. (2017). Report on the contextual determinants of child health policy. Available from http://www.childhealthservicemodels.eu/wp-content/uploads/Context-Culture-Report.pdf
Ziebland & Herxheimer (2008) Ziebland, S. , & Herxheimer, A. (2008). How patients’ experiences contribute to decision making: Illustrations from DIPEx (personal experiences of health and illness). Journal of Nursing Management, 16, 433–439.
- Prelims
- Chapter 1 The MOCHA Project: Origins, Approach and Methods
- Chapter 2 Models of Primary Care and Appraisal Frameworks
- Chapter 3 Listening to Young People
- Chapter 4 Child Centricity and Children’s Rights
- Chapter 5 Equity
- Chapter 6 The Limited Inclusion of Children in Health and Health-related Policy
- Chapter 7 The Invisibility of Children in Data Systems
- Chapter 8 The Conundrum of Measuring Children’s Primary Health Care
- Chapter 9 Measurement Conundrums: Explaining Child Health Population Outcomes in MOCHA Countries
- Chapter 10 Services and Boundary Negotiations for Children with Complex Care Needs in Europe
- Chapter 11 School Health Services
- Chapter 12 Primary Care for Adolescents
- Chapter 13 Workforce and Professional Education
- Chapter 14 e-Health as the Enabler of Primary Care for Children
- Chapter 15 Affiliate Contributors to Primary Care for Children
- Chapter 16 The Transferability of Primary Child Healthcare Systems
- Chapter 17 National and Public Cultures as Determinants of Health Policy and Production
- Chapter 18 Bringing MOCHA Lessons to Your Service
- Chapter 19 Evidence to Achieve an Optimal Model for Children’s Health in Europe
- Appendix 1: List of MOCHA Scientists
- Appendix 2: List of MOCHA Country Agents
- Index